






INFORMATION ON HEAD & NECK CANCERS
Cancer Awareness
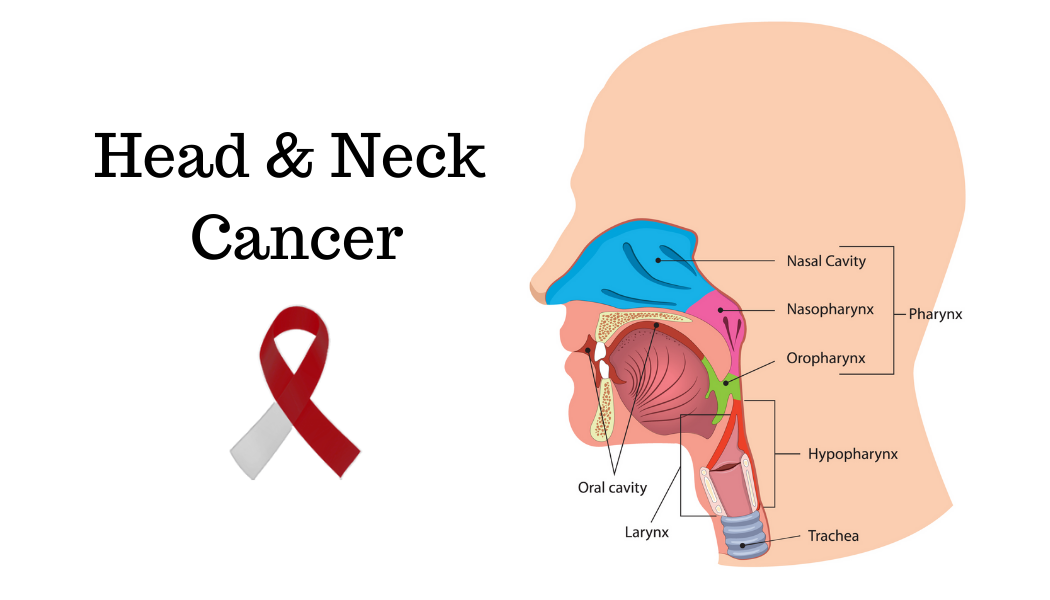
What are Head and Neck Cancers?
Head and neck cancer is a term used to
denote cancer that develops in the mouth, throat, neck, nose, sinuses,
salivary glands, thyroid or other areas of the head and neck. Most of
these cancers are squamous cell carcinomas, or cancers that begin in the lining
of the mouth, nose and throat. 85% of head and neck cancers are linked to
tobacco use, and 75 % are associated with a combination of tobacco and alcohol
use.
What are precancers?
The chronic
effect of carcinogens cause changes in the lining of the mouth. Features like
white patches (leukoplakia), red patches (erythroleukoplakia), tightening of
the mucosa (oral sub mucous fibrosis) or lace-like patches (oral lichen planus)
are called pre-cancers or pre-malignant conditions, and indicate that the
lining has started on its path to becoming cancerous. They can sometimes be
halted by stopping the addictions.
What causes Head and Neck Cancers? (Risk factors)
1. Tobacco in any form, whether smoked
(cigarettes, bidi, cigar, pipe etc.) or smokeless (gutkha, pudiya, gulmanjan,
soorti, paan masala etc.) is the strongest risk factor. The habit of stuffing
paan in the mouth while working long hours, is a unique risk factor mostly
found in the Indian subcontinent.
2. Alcohol acts as an independent risk factor, and also potentiates the effect of tobacco
by making its carcinogens more soluble, which can then be easily absorbed by
the lining of the oral cavity and oropharynx. Therefore, alcohol and tobacco
together are synergistic, not additive, ie 1+1=11, not 2.
How to suspect Head and Neck Cancers?
The mouth, throat and neck are the most common areas affected by head neck cancers. Symptoms depend on where the cancer develops and how it spreads. These tumours often cause symptoms that are similar to less serious conditions. So, these symptoms and signs are not diagnostic for throat cancer because many other problems like common cold, sinusitis or acid reflux can mimic head neck cancer. However, any person who develops these symptoms and has risk factors should immediately consult in the clinic.
- A non-healing ulcer in the mouth
- A lump in the throat or neck, with or without pain
- A persistent sore throat
- Trouble swallowing (dysphagia)
- Unexplained weight loss
- Frequent coughing
- Change in voice or hoarseness
- Ear ache or blocked ears
- A red or white patch in the mouth
- Bad breath that’s unexplained by hygiene
What are the treatment modalities?
There are many treatment modalities
available which are tailored to the patient’s site, type and extent of cancer.
The general fitness of the patient plays a role in his/her ability to tolerate
the treatment. The treatments mainly used are:
Surgery
- Tumor removal, also called curative or primary surgery: Surgery is used to remove the tumor and some of the nearby healthy tissues. The tissue around the tumor is called the margin. Tumor removal may be the primary treatment in some types of cancer and may be used as the sole treatment, or in conjunction with other modalities, such as chemotherapy or radiation therapy.
- Salvage surgery- Patients whose disease recur after treatment with chemotherapy and/or radiation therapy are treated with salvage surgery. There is an extremely small window of opportunity for such patients, and they must be evaluated promptly.
- Diagnostic Procedures: A biopsy may be used to diagnose certain cancers. During a surgical biopsy, the surgeon makes an incision into the skin to remove some or all of the suspicious tissue. This is sent to the pathologist to examine the tissue and diagnose the type of tumor, which dictates further treatment.
Radiation Therapy - Radiation therapy is the use of high-energy x-rays or other
particles to destroy or shrink cancer cells. A doctor who specializes in giving
radiation therapy to treat cancer is called a radiation oncologist. A radiation
therapy regimen, or schedule, usually consists of a specific number of
treatments given over a set period of time, and maybe used either as the sole
modality or in conjunction with surgery, chemotherapy or immunotherapy.
Chemotherapy - Chemotherapy is the use of drugs to destroy cancer cells. It acts on
all rapidly growing cells, but more so on the cancer cells. Therefore, they can
also cause damage to healthy cells, which account for the side effects of
chemotherapy. The types of chemotherapy are:
- Neoadjuvant
- Before surgery, to shrink tumors, and make
it operable.
- Adjuvant (usually along
with radiation) - After surgery, to consolidate the gains of surgery.
- Curative - To treat
cancers of the blood or lymphatic system, such as leukemia and lymphoma.
- Palliative - For cancer
that comes back after treatment, called recurrent cancer, or for cancer
that has spread to other parts of the body, called metastatic cancer.
Immunotherapy- Immunotherapy is a type of cancer treatment. It uses substances made
by the body or in a laboratory to boost the immune system and help the body
find and destroy cancer cells. Immunotherapy can treat many different types of
cancer. It can be used alone or in combination with chemotherapy and/or other
cancer treatments.
The U.S. Food and Drug Administration (FDA)
has approved two types of immunotherapy to treat head and neck cancer:
nivolumab and pembrolizumab. These drugs are checkpoint inhibitors, and they both
work in a similar way by taking the foot off one of the brakes of the immune
system, called PD-1.
What are the after effects of
treatment of head neck cancers?
Head neck cancers affect the most critical
aspects of speech, swallowing, smell and appearance. Therefore, its treatment
also has implications in the day-to-day activities of the patient.
Due to surgery:
- Changes in breathing- Occasionally, some people need a tracheostomy, which is an opening of the trachea directly onto the skin, kept open by a tracheostomy tube. It may be temporary or permanent, depending on the disease. Some patients may also need a feeding tube on a temporary or permanent basis.
- Changes to
appearance- There will be surgical scars on the
face and/or neck, which are permanent. Attempts will be made to keep the
scars hidden in skin creases or do the surgery trans-orally, but this may
not always be possible. If part of the jaw, nose or skin is removed, the
face will look different. Reconstruction with a prosthesis, local flap,
regional flap or free flap will restore the appearance to a great extent.
- Changes in
speech- In tongue cancers, lip cancer, cheek
cancer, jaw cancer, certain consonants will not be clearly pronounceable
depending on the site and extent of surgery. In total laryngectomy, the
voice box is removed, and the patient can be rehabilitated by other means.
- Changes in eating- Chewing and swallowing involves lips, teeth, tongue and the muscles in mouth, jaw and throat working together. Patients with a head and neck cancer have difficulty swallowing (dysphagia) before, during or after treatment. A temporary nasogastric tube is almost always placed after a major head neck surgery, but eating patterns do change depending on the site and extent of surgery. Maneuvers to overcome these difficulties will be taught to the patient as he/she recovers from the surgery.
Due to chemotherapy and radiation therapy:
Common side-effects of
chemotherapy include - Mouth ulcers, nausea, vomiting, weakness, loss of hair,
diarrhea, fever, loss of appetite, electrolyte imbalance etc.
Radiation therapy causes
dryness of mouth, difficulty in chewing, difficulty in swallowing, dental
caries (saliva is protective) and altered taste sensation, but these are
minimized nowadays due to sophisticated radiation techniques. If the patient
needs these modalities, he/she will be referred to the concerned specialist,
who will explain the implications in greater details.
General Workup Needed For Diagnosis
/ Staging & Treatment Plan
All
patients with suspected carcinoma of head and neck should be evaluated and
should record the following:
A. History
B. Clinical Examination Performance
C. Nutrition status assessment
D. Histological diagnosis – FNAC/Biopsy/ Slide
review
E. Imaging for extent of disease and assessment
of operability
F. Clinical staging and
G. Documentation of the subsite(s)
involvement
H. Investigations
- EUA / Endoscopy for mapping of disease
- USG for N0 neck in select case
- PET - CT whenever indicated
X-Ray Chest CT Scan / MRI for extent of disease
Treatment decisions for all patients is
made in a multidisciplinary joint clinic with the goal for maximizing survival
and preservation of form and function.